
The European Association for the Study of the Liver (EASL) and The Lancet have published a landmark report on liver disease in Europe. In this brand new EASL-Lancet Liver Commission a multi-disciplinary group of experts calls for a paradigm shift in the liver disease response in Europe: prevention and early detection, not end-stage treatment of complications.
In response, Movendi International supports the call for a paradigm shift and calls for greater focus on the potential of alcohol policy to prevent liver disease and promote health for all.
Liver disease is now the second leading cause of years of working life lost in Europe. The Liver Commission addresses the major contribution of alcohol to Europe’s liver disease burden. And the Liver Commission issues a strong call for European governments to introduce uniform alcohol policy solutions to prevent and reduce alcohol harm, including a complete ban of alcohol advertising, sponsorship, and promotion – also in social and digital media.
We congratulate EASL and The Lancet for the comprehensive work. Movendi International welcomes the bold and ambitious recommendations in the brand new Liver Commission and we strongly support the call for a paradigm shift in the European response to the liver disease burden,” says Kristina Sperkova, International President of Movendi International, the largest global social movement for alcohol prevention and control.
Kristina Sperkova, International President, Movendi International
The coronavirus pandemic reminds us all just how important health and well-being really are. A healthy Europe where all people can lead healthy and fulfilling lives is an important priority for people. We want to live in healthy environments and we want our loved ones to live long lives in good health.
But high levels of alcohol use and harm cause a heavy burden. For example, in Europe, alcohol consumption is by far the leading cause of liver-related deaths. Alcohol-related liver disease is the most frequent type of liver disease, responsible for at least 50% of cirrhosis cases.
Europe has the highest level of alcohol use in the world. Together with ultra-processed food and high prevalence of obesity, the products and practices of the alcohol industry are the major drivers of liver-related death and disease. More than 50% of end-stage liver disease is due to heavy levels of alcohol consumption – and the alcohol industry makes large parts of their profits from heavy alcohol consumption.
In her keynote speech at the launch of the landmark report, President of the European Commission, Ursula von der Leyen, emphasized the importance of prevention of chronic diseases in general and liver disease in particular, to promote health, well-being, and greater quality of life for all Europeans.
- Europe has the highest rates of alcohol consumption per person, the highest prevalence of heavy episodic alcohol use, and the lowest rates of alcohol abstention in the world.
- Alcohol combines with obesity and other risk factors for liver disease to drive the current high rates of end-stage liver disease and liver cancer.
- Alcohol causes about 40% of the 287,000 premature liver-related deaths in Europe every year, although the true number might be higher.
Far beyond the liver, alcohol and ultra-processed foods represent key health challenges in the 21st century, and it is increasingly clear that liver disease acts as a cipher for health and a sentinel for our public health capacity.
The EASL-Lancet Liver Commission report is an important milestone highlighting the harm that the products and practices of the alcohol industry cause to our communities.
We see in the new data, what we know from our experiences in our families and workplaces, in our football clubs and book clubs, in our high-school reunions: alcohol is fueling a massive loss of healthy years of life. Our members who live in countries from all around Europe are very concerned about alcohol industry tactics and the harm they cause to every family and community.
If nothing happens, liver disease deaths alone will cause healthy life expectancy to decline by 1.3 years over the next 30 years, with 46% of the decline due to alcohol and 28% as result of obesity.
The important lesson from the Liver Commission is: there are solutions available and they are highly impactful and well proven.”
Kristina Sperkova, International President, Movendi International
The Liver Commission outlines how Europe can advance prevention with the implementation of effective policy action on taxation, food reformulation, and product labelling, advertising, and availability, similar to that implemented for tobacco, to reduce consumption of alcohol, ultra-processed foods, and foods with added sugar, especially among young people.
Out of its ten bold and ambitious recommendations, two are focused on alcohol prevention and control:
- European governments must introduce uniform policies to reduce harm due to alcohol.
- A complete social and digital media ban on the marketing of alcohol and ultra-processed, high-fat and high-sugar foods targeted to children.
The Liver Commission emphasizes that with regards to alcohol, the evidence for equitable public health policies is remarkably consistent, summarised by WHO as the alcohol policy best buys:
- Tax increases on alcohol-containing beverages,
- Comprehensive restrictions and bans on alcohol marketing, and
- Restrictions on the availability of retailed alcohol.
Alcohol policy solutions hold vast and largely untapped potential to prevent and reduce liver disease.
People have a right to be protected from alcohol marketing. And raising the price of alcohol in Europe through modern alcohol excise taxes will reduce the liver disease burden, promote health, and raise domestic resources for investments in better healthcare.
The paradigm shift towards prevention should be driven by a region-wide initiative for alcohol taxation, and new investments in implementing the WHO’s SAFER alcohol policy blue print.”
People consistently value health as the most important condition for a happy and fulfilled life. And alcohol policy solutions are powerful catalysts for preventing harm and promoting health.
Notes to the editor
About Movendi International

With 135 Member Organization from 54 countries, Movendi International is the largest independent global movement for development through alcohol prevention. We unite, strengthen and empower civil society to tackle alcohol as serious obstacle to development on personal, community, societal and global level.
About the EASL-Lancet Liver Commission
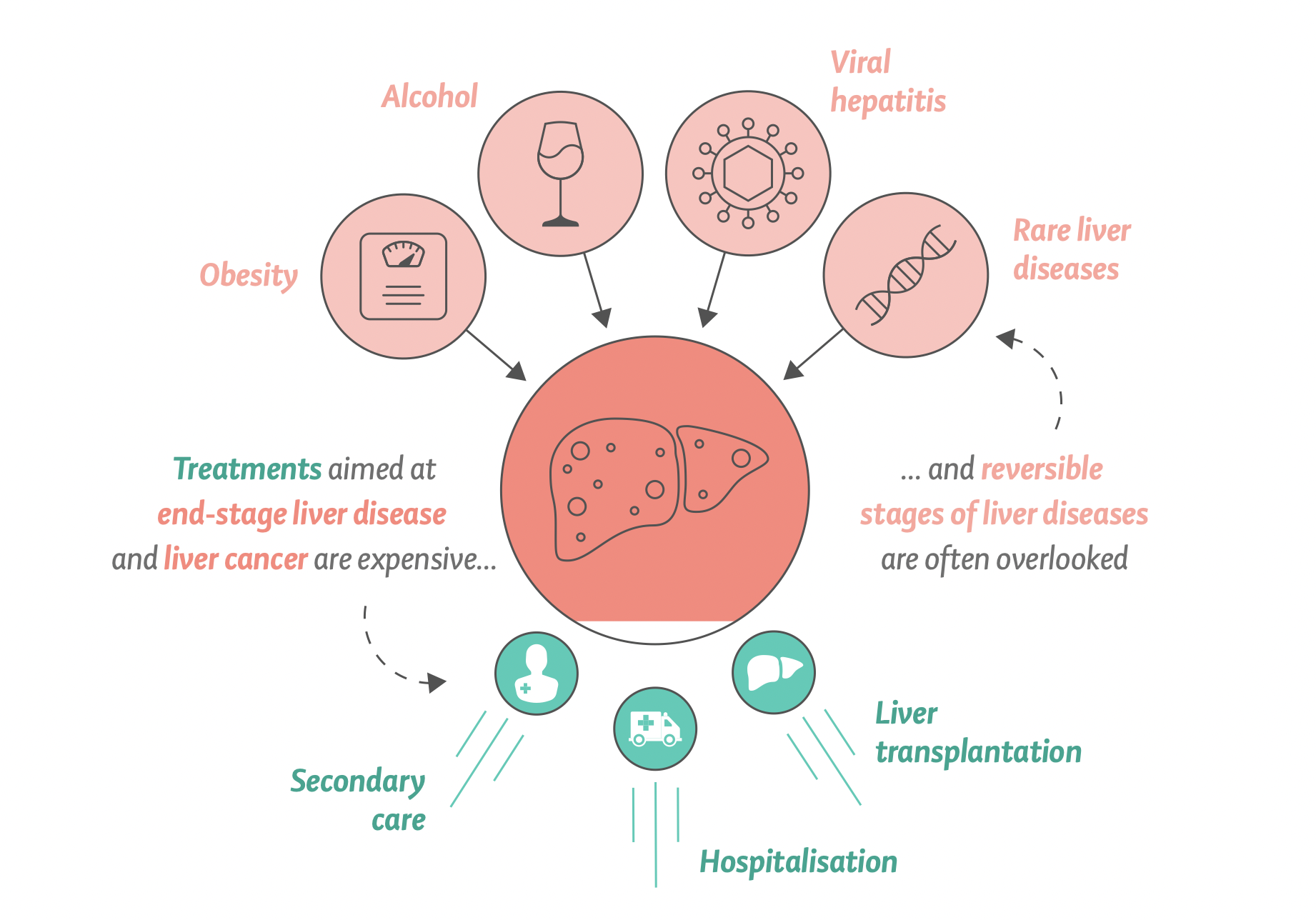
Liver disease is a leading cause of years of working life lost in Europe, second only to ischaemic heart disease. One of the continuing problems has been the focus on end-stage liver disease and its complications – cirrhosis and cancer.
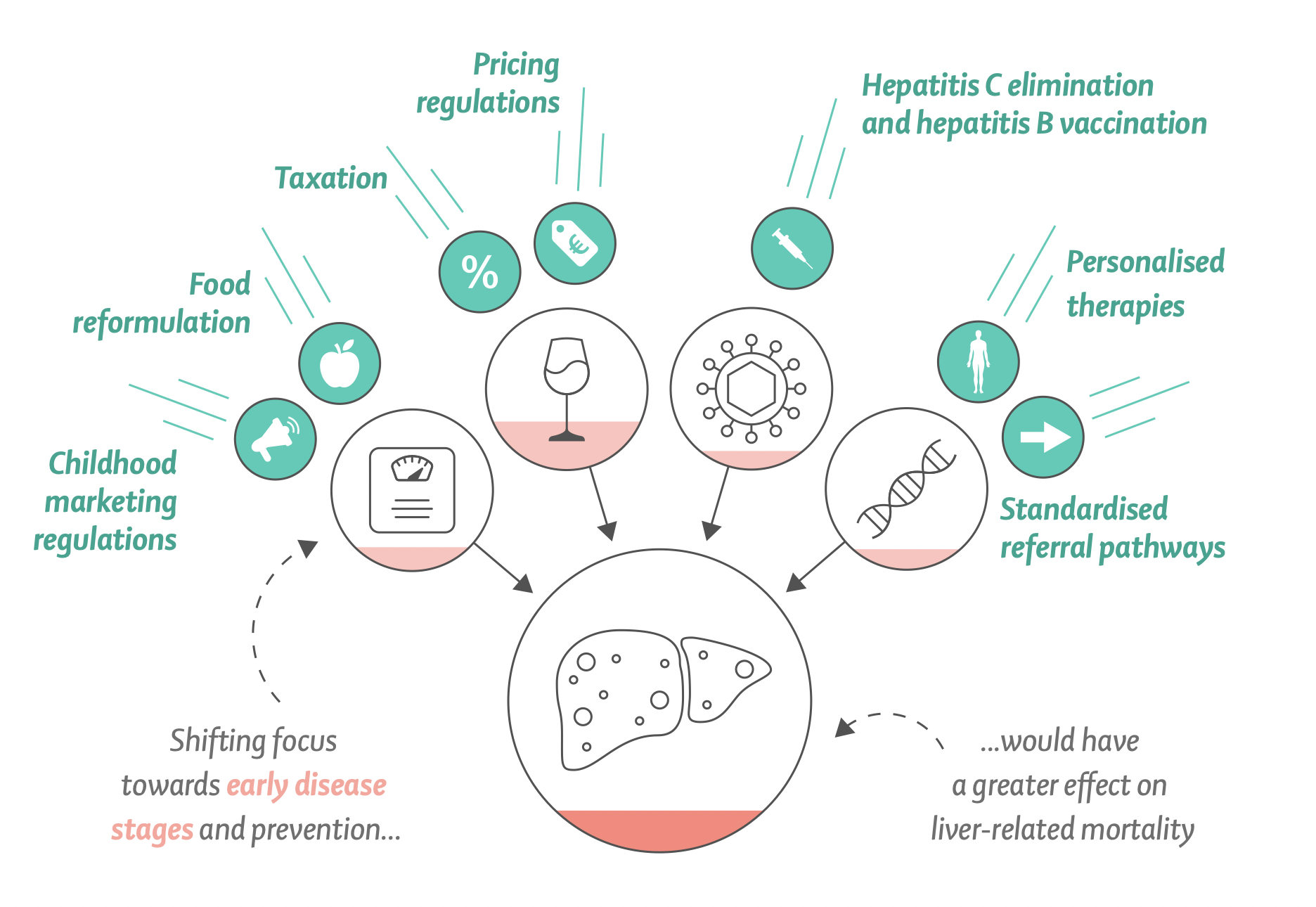
The Commission argues that there should be a fundamental change to prevent the development of advanced liver disease by embracing simple methods for early identification of progressive liver fibrosis together with strategies for disease prevention.
Underserved and marginalised communities, including children, require particular attention, and the significant stigma associated with liver disease needs tackling including the removal of stigma-associated terms in medical nomenclature.
Policy actions for marketing, pricing, and taxation of alcohol and unhealthy foods are of vital importance for supporting and preserving liver health.
How the Liver Commission addresses alcohol harm and alcohol policy solutions can be read in greater detail here.
Key facts – Liver Commission and alcohol overview
The Liver Commission says targeting end-stage liver disease with high-cost interventions is less effective at reducing liver-related mortality. Instead, the Liver Commission recommends a strategy focused on tackling the main causes of liver disease. Such an approach was cheaper to implement, and had a substantially greater effect.
Mortality from alcohol-related liver disease is substantially greater for disadvantaged socioeconomic groups, particularly for younger patients, resulting in major health inequalities.
The COVID-19 pandemic has also brought with it physical restrictions that might create environments that lead to increased alcohol consumption. Recently, a U.S. study provided evidence for an alarming increase in Alcoholic Hepatitis associated with increasing heavy alcohol use during COVID-19 and highlighted the need for public health interventions around heavy alcohol consumption.
Such change in liver disease and deaths are entirely consistent with increases in alcohol consumption predominantly impacting on those with the highest alcohol intake. The case for action for liver disease is even stronger as a result.
Europe has the highest rates of alcohol consumption per person the highest prevalence of heavy episodic alcohol use, and the lowest rates of abstention from alcohol in the world. Alcohol combines synergistically with obesity and other risk factors for liver disease to drive the current high rates of end-stage liver disease and liver cancer. Alcohol causes about 40% of the 287,000 premature liver-related deaths in Europe every year, although the true number might be higher.
The OECD model projects:
- Healthy life expectancy to be ca. 1.3 years lower over the next 30 years because of deaths due to liver diseases, with 46% of the reduction as a result of alcohol consumption and 28% as a result of obesity.
- The average annual health expenditure for liver disease in the EU27 + 5 countries is €4.3 billion.
- The impact of liver disease on the economy of the same group of countries leads to the loss of the equivalent of 5 million full-time workers per year.
In Europe, chronic liver disease has a substantial impact on young and middle-aged individuals in their prime working years, with the peak age of death occurring in the late 40s and early 50s. This contrasts with mortality from smoking-related and other obesity-related illnesses, such as lung cancer or type 2 diabetes, for which deaths typically occur in the 60s and 70s.

Age distribution of deaths in Europe due to alcohol-related liver disease
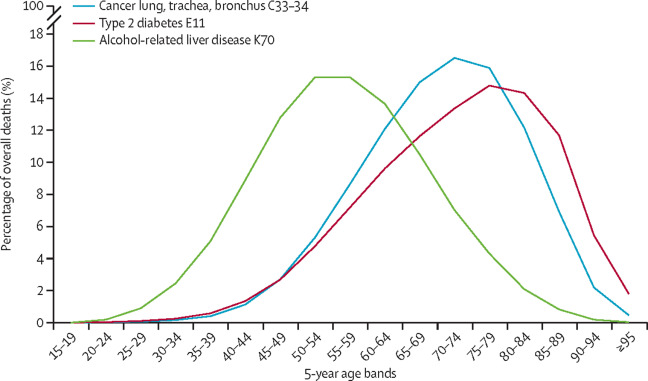
Consequently, data from the World Health Organization shows that liver disease is now second only to ischemic heart disease as the leading cause of years of working life lost in Europe. On average, two-thirds of all potential years of life lost due to mortality from liver diseases are years of working life.
Alcohol policy solutions to prevent and reduce the liver disease burden in Europe
The Liver Commission outlines how Europe can move forward with implementation of effective policy action on taxation, food reformulation, and product labelling, advertising, and availability, similar to that implemented for tobacco, to reduce consumption of alcohol, ultra-processed foods, and foods with added sugar, especially among young people.
With regards to alcohol, the evidence for equitable public health policies is remarkably consistent, summarised by WHO as best buys:
- Tax increases on alcohol-containing beverages,
- Comprehensive restrictions and bans on alcohol marketing, and
- Restrictions on the availability of retailed alcohol.
Alcohol tax increases and minimum unit price for alcohol have implementation costs that are lower than the corresponding benefits in reduced health expenditure and increased labour force productivity. Alcohol taxes also generate revenues.
More details on how the Liver Commission addresses alcohol harm and policy solutions
- In Europe, alcohol consumption is by far the leading cause of liver-related mortality.
- Europe has the highest levels of alcohol consumption per person, the highest prevalence of heavy episodic alcohol use, and the lowest rates of abstention from alcohol in the world.
- Alcohol was responsible for around 580,000 deaths in 2019 (6.2% of all deaths) in the WHO European region, according to the Global Burden of Disease study modelling.
- Alcohol causes about 40% of the 287,000 premature liver-related deaths in Europe every year,
- but the true number is probably higher.
- Alcohol-related liver disease is the most frequent type of liver disease, being responsible for at least 50% of cirrhosis cases, and is the most common indication for liver transplantation in Europe.
- Nevertheless, research on alcohol-related liver disease is underrepresented, amounting to just 5% of all publications in the area of liver disease (2010–14 assessment).
- At the large European and American liver congresses, alcohol-related liver disease represented only 7% and 4%, respectively, of the research presented.
- Alcohol-related harm correlates with the volume and pattern of alcohol use, with epidemiological studies showing an exponential dose–response relationship between alcohol and liver disease.
- For most countries in the WHO European region, there is a strong correlation between liver-related mortality rates and population-level alcohol consumption.
- The evidence linking liver-related mortality and population-level alcohol consumption sends a crucial message for disease prevention:
- alcohol-related cirrhosis is a dose-related condition at the population level, and the most effectual and cost-effective means to reduce mortality rates from alcohol-related liver disease are interventions that reduce population-level alcohol consumption.