
Alcohol control policies reduce all-cause mortality in Baltic Countries and Poland between 2001 and 2020
Research article
Abstract
Alcohol consumption in the Baltic countries and Poland is among the highest globally, causing high all-cause mortality rates. Contrary to Poland, the Baltic countries have adopted many alcohol control policies, including the World Health Organization (WHO) “best buys”.
The aim of this study was to evaluate the impact of these policies, which were implemented between 2001 and 2020, on all-cause mortality.
Monthly mortality data for men and women aged 20+ years of age in Estonia, Latvia, Lithuania, and Poland were analysed for 2001 to 2020.
A total of 19 alcohol control policies, fulfilling an a-priori defined definition, were implemented between 2001 and 2020 in the countries of interest, and 18 of them could be tested.
Interrupted time-series analyses were conducted by employing a generalized additive mixed model (GAMM) for men and women separately.
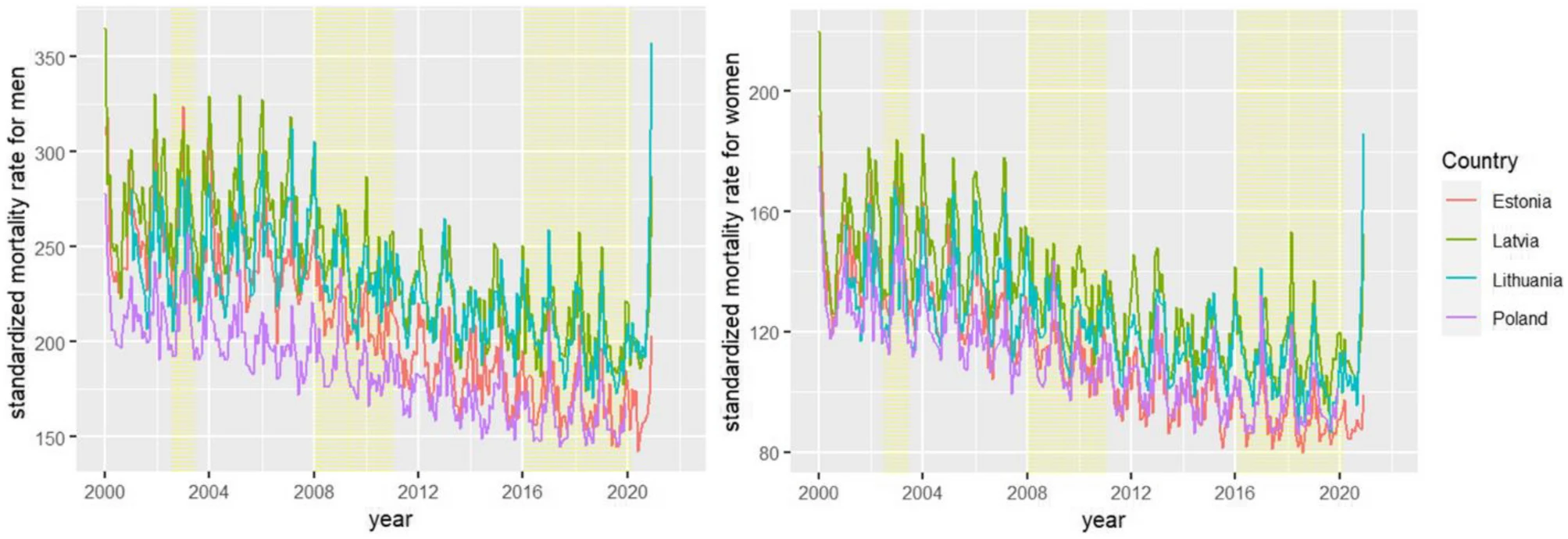
The age-standardized all-cause mortality rate was lowest in Poland and highest in Latvia and had decreased in all countries over the time period.
Taxation increases and availability restrictions had short-term effects in all countries, on average reducing the age-standardized all-cause mortality rate among men significantly (a reduction of 2.31%).
All-cause mortality rates among women were not significantly reduced (a reduction of 1.09%).
In conclusion, the alcohol control policies implemented between 2001 and 2020 reduced all-cause mortality among men 20+ years of age in Baltic countries and Poland, and thus, the practice should be continued.
Research highlights
The three Baltic countries implemented different levels of alcohol availability, affordability, and marketing restrictions in the past 20 years. Poland on the other hand established only a taxation increase in 2020, and even loosened control in 2002 via a decrease in alcohol excise taxation.
Some of these effects have been evaluated such as the 2017 alcohol control policy of increased excise taxation implemented in Lithuania. However, a single evaluation of an alcohol control policy is subject to potential confounding by other events and conditions which may have happened at the same point in time. Thus, researchers need to introduce as much control as possible; analysing several interventions in different countries in the same region allows for such control, and aids in determining the general impact of policies by aggregating effects across various time points and conditions.
As the Baltic countries and Poland differ in the implementation degree of alcohol control policies and the time points when the policies were adopted, they constitute unique conditions to evaluate such effects, where the other countries can serve as control conditions.
Identified alcohol policy interventions
Concretely, the researchers identified all policies that had been implemented within a timespan of two decades, which fulfilled clear a priori defined criteria of decreased affordability and availability.
Simultaneously measuring their average effect allowed for:
- more generalizable estimates on average effect sizes of such policies;
- better control for secular trends across the region, since we can use the other countries as control conditions for each policy effect;
- better control of all other factors, as it is highly unlikely that, at exactly the same time of all 18 alcohol control interventions other events occurred which triggered the effects.
A total of 18 policies, classified as “best buys” and expected to have an immediate effect, were applied in the study period based on the following criteria:
- taxation increases should decrease affordability of alcoholic beverages (affordability was measured by data on alcohol prices, inflation and disposable income); and
- availability restrictions should reduce availability by at least 20% (decrease in opening hours at least 20%).
Prior analyses showed that these policies had an impact on consumption level.
In Estonia, eight policies were selected; Latvia, five policies; Lithuania four policies; and in Poland, one policy.
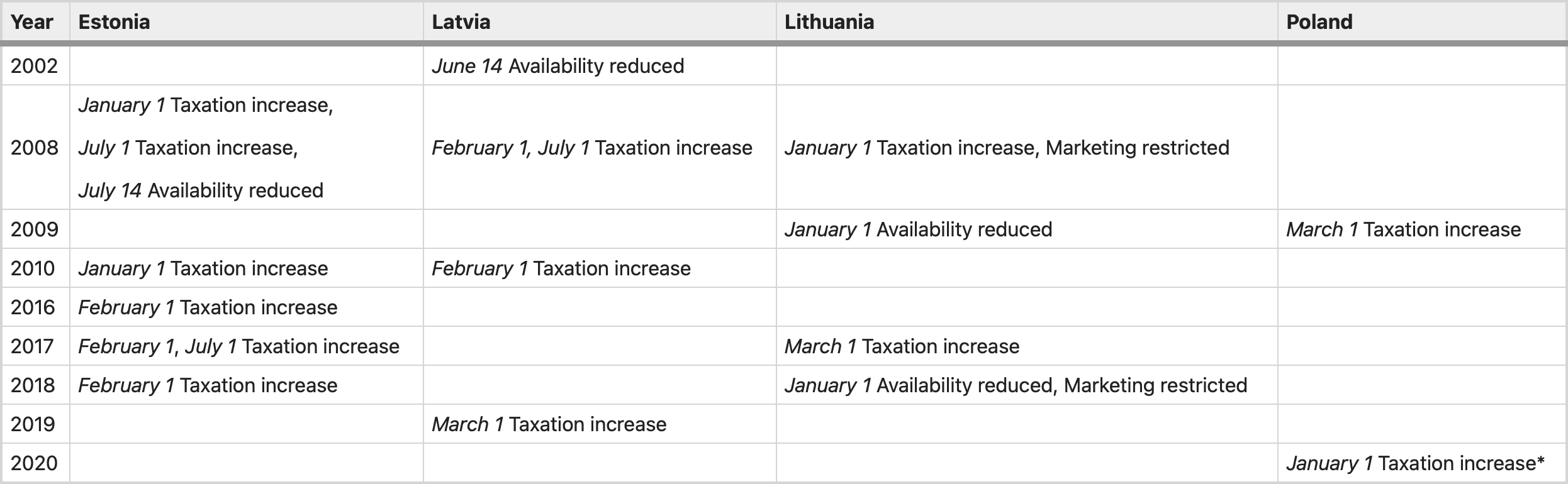
From: Alcohol control policies reduce all-cause mortality in Baltic Countries and Poland between 2001 and 2020 *This policy was not included in data analysis, because 2001–2019 Poland data were used. More details about all policies published before.
The policy implemented in Poland could not be tested due to a lack of data for 2020 for this country.
The effect was modelled to last for one year after implementation, and to test, whether other events at the same time in the country of implementation were impacting on the effect of the policy, the researchers tested interaction terms between the countries and policies.
One year was chosen as the time reference, as inflation and disposable income were expected to have an impact on affordability to diminish the impact of tax increases, and as we expected people to develop coping strategies to deal with availability restrictions.
Results
A total of 240 months of data were included in the analyses. The standardized mortality rates over time show a downward trend and evidence of seasonal variation. For both men and women, generalized additive mixed model (GAMM) confirmed that the standardized mortality rates decreased over time after adjustment.
Effects of alcohol policy
The policy effects estimated in the full and reduced models were similar. For example, the estimate for the policy effect for men was − 0.024 in the full model compared to − 0.023 in the reduced model, despite the fact that standard errors were larger in the full model due to more variables included.
In the final reduced model, alcohol control policies had a significant effect on the all-cause mortality rate among men (0.0228), which transformed into a reduction of 2.31% in all-cause mortality rate.
Given the different numbers of deaths in the countries, this corresponds to average effects of about
- 172 male deaths avoided per year for Estonia,
- 317 male deaths avoided per year for Latvia,
- 478 male deaths avoided per year for Lithuania, and
- 4340 male deaths avoided per year for Poland.
For females, the effect was not significant (0.0108), however because it approached a p < 0.05 threshold, we computed its effect, which transformed into 1.09%, corresponding to average effects of around
- 84 female deaths avoided per year for Estonia,
- 159 female deaths avoided per year for Latvia,
- 218 female deaths avoided per year for Lithuania, and
- 1892 female deaths avoided per year for Poland.
Alcohol policy effects of countries
For men, Latvia had a higher age-standardized all-cause mortality rate than Poland (by 38.82%).
Estonia and Lithuania also showed higher mortality than Poland: Estonia by 16.01% and Lithuania by 27.26%.
The interaction effects of countries with alcohol control policies in the full model were not statistically significant, which reflected that the policies did not change all-cause mortality rates differently among the four countries.
For women, compared with Poland, Estonia and Latvia also had higher age-standardized all-cause mortality rate: Estonia by 21.40% and Latvia by 8.93%.
Lithuania, on the other hand, had a significantly lower age-standardized all-cause mortality rate, by − 4.57% on average. Similar to men, the interaction effects between countries and policies in the full model were not statistically significant.
Figure 2 shows the mortality gains summed up over the 11 interventions in total and by broad causes of death.

Overall, men showed markedly more gains than women.
Differentiating by cause of death, ischemic heart disease had the largest mortality gains in mortality followed by injury, stroke and gastrointestinal disease.
All of these categories are causally linked to alcohol, and all of them are expected to change abruptly with changes in exposure, as evidenced by the changes in mortality due to the Gorbachev reforms.
As expected, there had been only minor changes in cancer mortality, in total comprising less than 5% of the total decrease. While certain cancers have been identified as causally impacted by alcohol use, this relationship has a long lag-time, so no immediate changes of the alcohol control measures were expected.
Conclusions
The alcohol control policies implemented in the Baltic countries and Poland were effective in significantly reducing all-cause mortality among men.
Given the difference in the number of deaths across countries, the reduction corresponds to average effects of about 172, 317, 478, and 4340 deaths avoided per year for Estonia, Latvia, Lithuania, and Poland, respectively. Analyses by cause of death in a subsample confirmed that the reduction was indeed based on alcohol-attributable causes of death.
With respect to all-cause mortality among women, the impact of implemented alcohol control policies was in the right hypothesized direction (i.e., a reduction); however, it was not statistically significant. As such, the results of the data analysis partially confirm the researcher’s hypothesis.
The results of this study contribute to other previous studies showing the effectiveness of alcohol control policies in reducing all-cause mortality, when the WHO “best buys” alcohol control policies were adopted.
Explanations for the differential impact on men and women
There are several explanations for the differential impact on men and women. Men are more likely than women to consume alcohol, they consume more alcohol when they consume, they have a higher prevalence of alcohol use disorders, and they are more prone to behavioural problems associated with acute alcohol consumption although women have a shorter time period between initiation of regular alcohol use and problem use compared to men and the gap between need and receipt of treatment is larger for women than for men.
In the WHO European Region the consumption of pure alcohol was four times higher among men compared to women in 2016, as a result the proportion of alcohol-attributable deaths was 12.3% among men and 7.8% among women.
It is possible that the stronger relationship between policies and all-cause mortality in men compared with women may be because alcohol accounts for a larger proportion of total mortality in men than in women.
Although alcohol control policies of taxation increase and availability reduction in the Baltic countries and Poland have been found to be effective in reducing alcohol per capita consumption of pure alcohol per year, future evaluation of the impact of these policies on specific population groups such as men and women would be important.
Life expectancy is determined by many factors, including demographic, economic, social, health system, and environmental factors. Also, health behaviours (like alcohol consumption) could have an impact on the average life expectancy of a country’s population. The average life expectancy of men and women also varied between the Baltic countries and Poland, the inequalities being particularly large in Baltic countries, for instance in 2019 the average life expectancy difference between men and women in Lithuania was 9.6 years (men—71.6 years, women—81.2 years), for comparison in Poland difference was 7.8 (men—74,1 years, women—81.9 years). As Stumbrys and colleagues indicated, positive changes in Lithuanian’s men life expectancy in 2007–2017 were result of decreased mortality from external causes of death, cardiovascular diseases and alcohol-related disorders. These causes are clearly related to alcohol consumption, and therefore alcohol control policies are expected to have an impact on them. Changes in women’s mortality were less related to alcohol consumption and mortality from external causes of death, therefore alcohol control policies had less influence on them. As a result, due to alcohol control policies implemented in Lithuania between 2008 and 2018, men’s age-standardized mortality decrease was higher compared to women. On the contrary, increase in alcohol consumption in Poland between 2002 and 2019 was found to be a feasible cause of slow down and then halted increase of life expectancy.
Impact of economic crisis
The economic crisis of 2008 which affected the Baltic countries at slightly different times (see above) contributed to a reduction of affordability of alcoholic beverages and was associated with a reduction of alcohol per capita consumption.
However, within an economic crisis or other crisis situation there may also be an increase in heavier alcohol users despite the overall volume of alcohol going down. Economic crisis has affected funding for the health systems by decreasing public expenditures on health care, which may have affected health indicators (life expectancy, all-cause mortality etc.) and public health was particularly affected in countries with highest recession.
Uniqueness of the study
The uniqueness of this study is that it evaluates the impact of immediately acting “best buy” alcohol control policies implemented in Estonia, Latvia, and Lithuania, on a broad measure, all-cause mortality, without distinguishing between policies and countries.
Poland was included in the analyses, but as a control country only, as the only alcohol control policies that met the a priori defined criteria implemented between 2000 and 2020 was outside the range of data available for analyses. Since the researchers included all instances of policy change, and still found impact on all-cause mortality, this indicates, that the “best buy” policies of taxation increases, and availability restrictions are still very valid and should be used more often to decrease all-cause mortality.
This study has demonstrated that alcohol control policies were associated with a reduction in all-cause mortality among men in the Baltic countries between 2001 and 2020. All-cause mortality among women also decreased, but not significantly so.