Strong Public Health interest in preventing under-age alcohol use
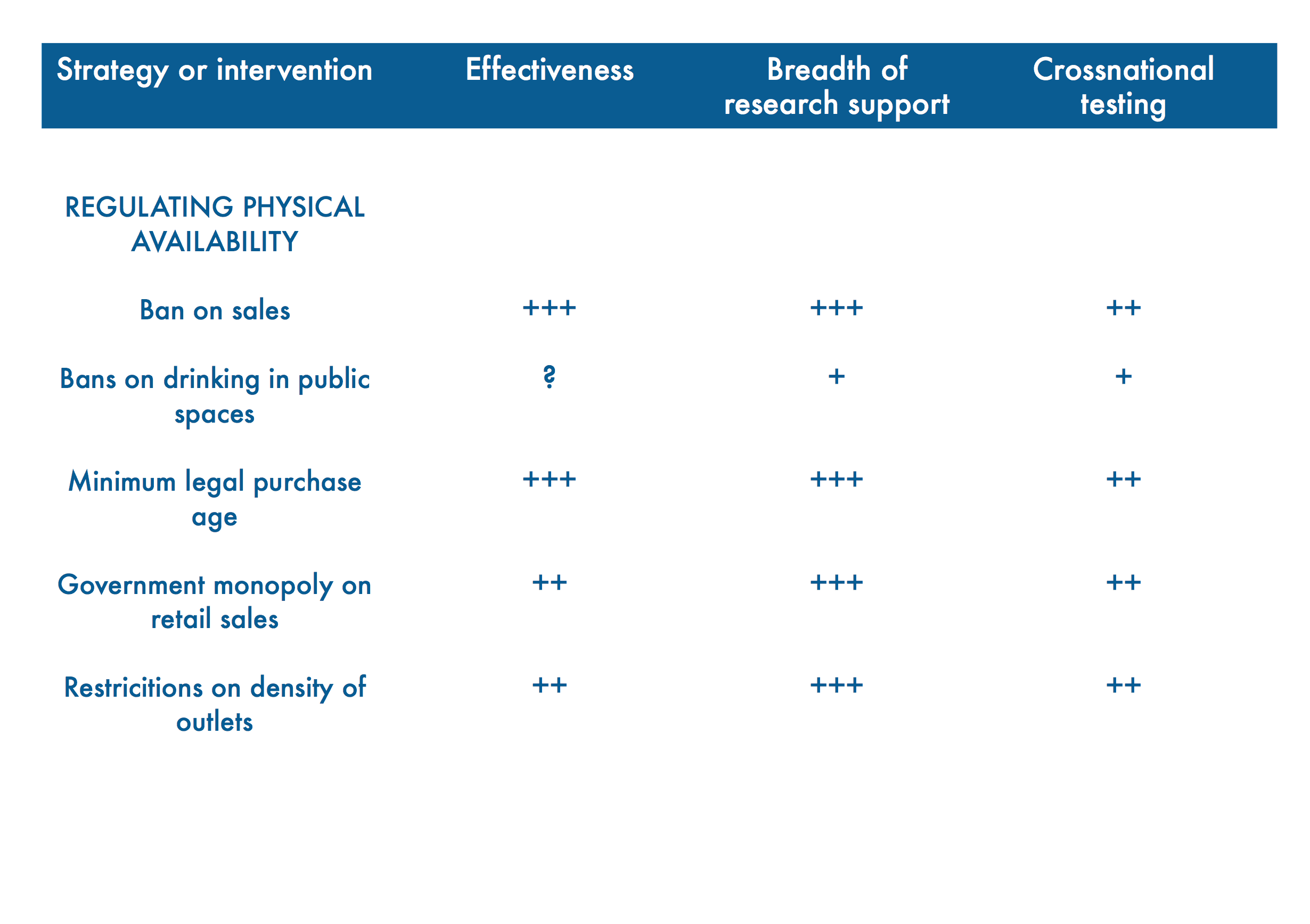
The WHO Global Alcohol Strategy outlines no less than 10 areas for action and intervention to prevent and reduce alcohol harm. Among those are the Three Best Buys in alcohol policy (regulating availability, affordability and marketing). Area 3 deals with “Community Action”. For this area the following policy option and intervention is recommended:
Mobilizing communities to prevent the selling of alcohol to, and consumption of alcohol by, under-age and to develop and support alcohol-free environments, especially for youth and other at-risk groups.”
Scientific evidence shows that early onset of alcohol use has long-lasting negative consequences.
Research by Grant and Dawson (via NIAA) shows:
People who reported starting to [use alcohol] before the age of 15 were four times more likely to also report meeting the criteria for alcohol dependence at some point in their lives.”
The earlier young people start to use alcohol, the worse the alcohol-related consequences:
- Alcohol dependence
- Traffic crashes
- Physical violence after alcohol consumption
- Other unintentional injuries after alcohol intake (e.g. drowning, falls)
- Potential damage to still-developing adolescent brain
- Lower chances of success in school
The bottom line is that society has a strong public health and social welfare interest in preventing under-age alcohol use.