Background
At the World Health Organization (WHO) Executive Board meeting in February 2020, member states, called for accelerated action on alcohol as a public health priority. A decision was adopted by unanimous consent (EB 146), requesting the WHO and its director-general to develop an action plan (2022-2030) to effectively implement the WHOs Global Alcohol Strategy as a public health priority.
Since then, WHO has conducted an extensive consultation process lasting two years, to develop the global alcohol action plan to accelerate alcohol policy development and implementation as public health priority – an urgent need according to WHO Member States. The consultation process included global and regional engagements with Member States, one informal meeting and web-based consultation with civil society and academia, and – controversially – also the alcohol industry, despite their fundamental conflict of interest.
The WHO Executive Board is made up of 34 technically qualified members. Every January, these members meet to agree on the agenda for the next World Health Assembly, including what resolutions should be considered, and how to implement decisions and policies.
This week between January 24 and 29, the 150th Session of the WHO Executive Board (EB150) meets and will discuss and adopt the new global alcohol action plan.
The proposed alcohol action plan will protect more people from the harms caused by the alcohol industry, save lives, improve livelihoods, and boost global outcomes for health and sustainable development.”
Kristina Sperkova, International President, Movendi International
EB150 has a packed agenda with 55 items and with 10 sub-items under agenda point 7, Non-Communicable Diseases (NCDs), where the alcohol action plan is included.
The alcohol policy agenda item (also known as ‘Annexes’ in reporting documents) can be found under item 7 of EB150, on the political declaration of the third high-level meeting of the UN General Assembly on the prevention and control of NCDs, see Annex 8, Appendix 1 for the alcohol action plan.
Quick links for participation
- Find all EB150 documentation here.
- Find the draft alcohol action plan, under so called “Appendix 1” to the report on the prevention and control of NCDs.
- Follow the EB150 discussions live here: Webcast.
- See which WHO Member States are currently members of the Executive Board.
- And find the preliminary timetable of EB150, here.
What did the 2020 Decision call for (EB146)?
In 2010, the World Health Assembly endorsed the WHO Global Alcohol Strategy. But since then, implementation of the global strategy has not resulted in meaningful reductions in deaths, diseases, and social and economic harms due to alcohol.
That is why in 2020, EB146 adopted a decision by unanimous consent that identified alcohol as a “public health priority”.
The decision contained four action points, requesting WHO and its Director General to:
- Develop an action plan (2022–2030) to effectively implement the WHO Global Alcohol Strategy as a public health priority;
- Develop a technical report on cross-border alcohol marketing, advertising and promotional activities, including those targeting youth and adolescents;
- Resource the work on alcohol harm and policy solutions adequately; and to
- Review the WHO Global Alcohol Strategy and report to the 166th session of the Executive Board in 2030 for further action.
The draft decision was originally proposed by Bangladesh, Bhutan, India, Indonesia, Islamic Republic of Iran, Philippines, the Russian Federation, Sierra Leone, Sri Lanka, Thailand and Viet Nam, with Norway and the European Union member states also jointly co-sponsoring the decision after compromise was reached.
Movendi International called the adoption of the decision “historic”. In a statement live from the World Health Organization Executive Board room, Movendi International said:
While the decision does not contain everything that communities around the world had hoped for, this decision today is a significant improvement.
It strengthens the global infrastructure for alcohol prevention and control. And it puts focus on the need for accelerating action.”
Maik Dünnbier, Director of Strategy and Advocacy, Movendi International
It had taken ten years for a substantive discussion of the global alcohol burden and the necessary policy response at the WHO governing bodies. The EB146 decision finally changed this. Since then, alcohol policy has been on the agenda over the last two years – and it is crucial that alcohol policy remains a regular agenda item in the coming years.
EB146 decision also illustrated growing awareness of the heavy burden that alcohol harm places on a broad range of health and development goals. The decision also underlined the growing commitment to take much more ambitious actions to protect people from harms due to alcohol.
In February 2020, commenting on the decision, Maik Dünnbier told Health Policy Watch:
It is also clear that more must be done: The action plan needs to be filled with bold targets and actions to turn the tide on alcohol harm.”
Maik Dünnbier, Director of Strategy and Advocacy, Movendi International
The draft of the action plan, developed based on the mandate from the EB146 decision, is now provided as an Appendix to Annex 8, under the NCDs agenda item at EB150.
What’s at stake? Facts and figures about alcohol harm and alcohol policy
The products and practices of the alcohol industry cause an unprecedented global disease and development burden. Globally, levels of alcohol consumption and alcohol-attributable harm remain unacceptably high. And the products and practices of the alcohol industry adversely affect 14 of 17 Sustainable Development Goals.
The Global Burden of Disease study for 2019 found that failure in tackling preventable non-communicable diseases has made the world more vulnerable to COVID-19. The study highlighted worrying data about alcohol’s contribution to the global burden of disease.
Alcohol remains one of the leading risk factors contributing to the global burden of disease. It is the eight leading preventable risk factor of disease. The contribution of alcohol to the global disease burden has been increasing from 2.6% of DALYs* in 1990 to 3.7% of DALYs in 2019.
Lack of progress and failure to implement high-impact alcohol policy solutions
Evidence shows that alcohol policy development has been ineffective over the past decade of the WHO Global Alcohol Strategy. For example, technical support to governments has been inadequate, and concrete technical tools have still not been developed. The WHO Secretariat has not allocated adequate resources for the work on alcohol harm. Efforts to protect country initiatives for alcohol policy development have also been inadequate, so that the alcohol industry could interfere, delay and derail such initiatives.
Overall, trends in alcohol consumption, alcohol’s contribution to the global burden of disease, and progress towards global targets are all pointing the wrong direction.
- Progress in the formulation and implementation of national and local alcohol policy solutions has been insufficient.
- Most countries, especially low- and middle-income countries (LMICs), have NOT implemented a comprehensive set of alcohol policies.
- No low-income country has reported increasing resources for implementing alcohol policy in the last decade.
- Many countries are failing to implement the alcohol policy best buy solutions, with LMICs more likely to have fewer evidence-based and cost-effective policies.
- Modelling forecasts that global targets to reduce alcohol use and harm will not be met.
- Without action, Africa could see an increase in both the absolute number and proportion of people consuming alcohol, the amount consumed per capita and heavy episodic alcohol use.
- South East Asia has seen a 29% increase in per capita alcohol use since 2010.
Alcohol affordability
- 95% of reporting countries implement alcohol excise taxes.
- Few use such taxes as a public health policy to reduce consumption.
- Less than half use price strategies such as adjusting taxes to keep up with inflation and income levels, imposing minimum pricing policies, or banning selling below cost or volume discounts.
Alcohol availability
- Less than one-third of countries have regulations on outlet density and days of alcohol sale.
- Some countries, mainly LMICs in Africa, still have no legal minimum purchase age.
Alcohol marketing
- Most countries have some policies on alcohol advertising.
- Alcohol marketing regulation continues to lag behind technological innovations and e-commerce, including rapidly developing new delivery systems.
- Most of the countries that reported no restrictions across all media types were located in the African or Americas regions.
Analysis of the global alcohol action plan
Based on Movendi International’s analysis of the flaws and shortcomings of the WHO Global Alcohol Strategy, we advocated for 11 key points to develop an ambitious and bold global alcohol action plan.
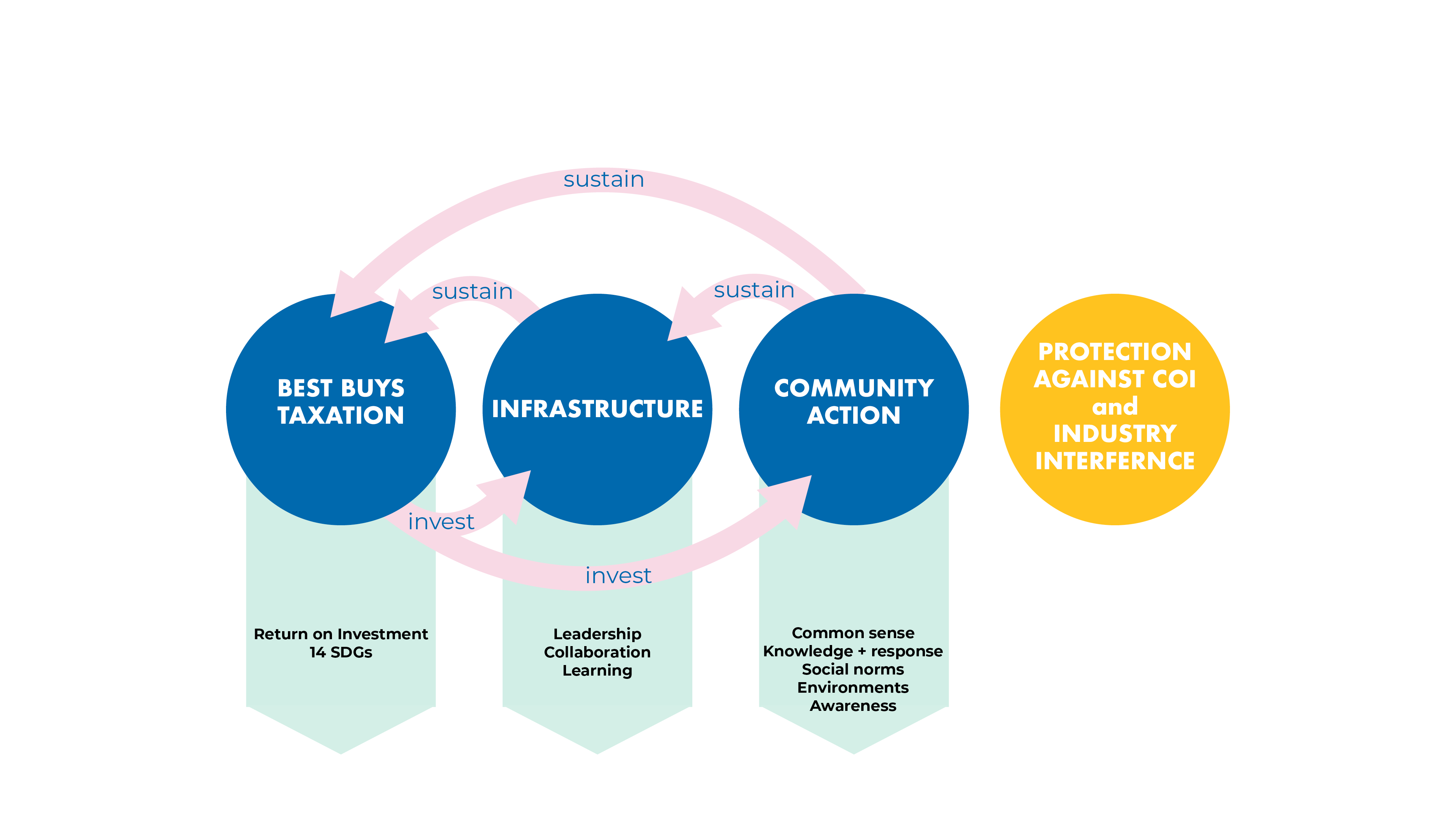
The focus is on how to facilitate and improve country action to protect more people through alcohol policy solutions. To achieve this, three elements are essential in the action plan:
- Making a difference on the country and community level through the alcohol policy best buys, and through bold and ambitious targets,
- Protecting alcohol policy development against conflicts of interest and alcohol industry interference, and
- Improving the global, regional, and national infrastructure for alcohol policy development and implementation.
As the analysis shows above, implementation of the alcohol policy best buys has been inadequate in the last ten years and needs to be accelerated. The alcohol industry remains the biggest obstacle to evidence-base public health action on alcohol. And the absence of robust infrastrcuture on all levels undermines sustained action, leadership, exchange, and accountability.
- Ensure bolder targets and bigger ambition,
- Craft stronger conclusions evaluating the decade of WHO GAS implementation,
- Better consider the needs of the most vulnerable and devise stronger actions to protect those at risk of being left behind,
- Improve and enhance the structure and apply best practices from other WHO action plans,
- Ensure greater focus on the SAFER strategies,
- Facilitate country action,
- Don’t normalize Big Alcohol through the global alcohol action plan,
- Ensure greater focus on governance and infrastructure improvements,
- Improve resourcing as well as reporting and review of implementation,
- Update nomenclature in line with state-of-the-art evidence, and
- Convene an Expert Committee.
Based on these key points, we have analyzed the WHO global alcohol action plan, now before EB150 recommended for adoption.

Movendi International welcomes and endorses the WHO draft Global Alcohol Action Plan.
The draft alcohol action plan contains several important elements to accelerate action on alcohol as public health priority – which Member States have called for in the decision at EB146.
Nevertheless, the members of Movendi International remain deeply concerned about the role the alcohol industry is given in the draft and about alcohol industry interference in the development of the global alcohol action plan.
Flaws of proposed action plan
The draft action plan still affords a role to the alcohol industry, still maintains WHO’s dialogue with the alcohol industry, and still maintains the flawed and outdated concept of “harmful use of alcohol”. These are serious shortcomings of the alcohol action plan and might jeopardize urgently needed acceleration of action to protect people from the harms caused by the alcohol industry.
Flaw #1: The Global Alcohol Action Plan normalizes the alcohol industry.
There are three problems:
- The role of the alcohol industry in the action plan
- The WHO dialogue with the alcohol industry
- The concept of “harmful use of alcohol”
Movendi International strongly disagrees with the role assigned to the alcohol industry in the global alcohol action plan, especially in the key areas for global action. The abundance of “measures” assigned to the alcohol industry across the action areas is problematic and this language is riddled with conflicts of interest and risks legitimizing alcohol industry involvement.
Movendi International advocacy asks:
The alcohol industry should not be assigned any role, action, or measure in the policy response to the harm that their own products and practices are causing.
In the action plan, the alcohol industry should be dealt with in a single paragraph, addressing conflict of interest; and that the alcohol industry is interfering against WHO-recommended alcohol policy solutions.
The action plan should be much clearer about spelling out the fundamental conflict of interest inherent in any involvement of the alcohol industry in public health-oriented alcohol policymaking.
The action plan should focus on substantial action to protect alcohol policy development from alcohol industry interference.
The Action Plan should clearly recommend total bans or comprehensive restrictions on alcohol advertising, sponsorship, and promotion across all platforms, instead of a partial elimination of marketing to minors and other “high-risk groups” by the alcohol industry.
Examples of problematic content:
- The term “economic operators” is mentioned 24 times throughout the action plan, however, the term “community” is only mentioned 9 times.
- But “community action” is actually one of ten areas of the WHO Global Alcohol Strategy – indicating the imbalance in the action plan towards the alcohol industry.
- Measures for alcohol industry in every action area.
- Under action area 2 (page 18), the action plan recommends self- and co-regulation of marketing and advertising.
- Action areas 1, 3, 6 for the WHO Secretariat (area 1), Member States (area 3), and economic operators in the alcohol industry (area 6) address conflicts of interest but this is not a substantial, clear way of spelling out conflict of interest concerns and protective measures against it.
The conflict of interest between alcohol industry profit interests and member states’ call to make alcohol policy a public health priority is fundamental and direct.
Alcohol industry interference against public health action to prevent and reduce alcohol harm has been identified by Member States as the biggest obstacles to country action on alcohol policy, according to the regional consultations with WHO member states.
Flaw #2: The Global Alcohol Action Plan maintains WHO dialogue with alcohol industry
Due to their fundamental, direct, and irreconcilable conflict of interest, the alcohol industry has not lived up to their self-regulatory objectives. Instead, it is actively working against them.
WHO’s engagement with the alcohol industry has not yielded any public health gains but has been used by the alcohol industry to re-cast their image as a legitimate stakeholder in policymaking and interfere in effective implementation of the WHO Global Alcohol Strategy.
Movendi International advocacy asks:
WHO should desist with dialogues with the alcohol industry whose interests’ conflict with those of public health. In the same manner that WHO does not engage with the tobacco industry and abides by the International Code of Marketing of Breast-milk Substitutes, WHO should cease this harmful practice of annual dialogue meetings that does not serve public and global health, but instead can be seen to help advance the alcohol industry’s profit maximization interest.
Examples of problematic content:
- In OP18, WHO specifies the dialogue with the alcohol industry (pages 18-19)
- WHO Secretariat Action 7 under area 3 (page 20) stipulates the Secretariat should organize “regular global dialogues” with the alcohol industry, in line with FENSA, focused on “industry partners’ contribution to reducing harmful use of alcohol as developers, producers, and distributors/ sellers of alcoholic beverages.”
- WHO Secretariat Action 6 under area 5 (page 28) makes it look like the alcohol industry dialogue has the same importance as collaboration with international organizations on data collection.
Some language has improved and become more robust with regards to conflict of interest considerations (Action areas 1 and 3). But all in all, this language cited above belongs to the most problematic parts of the alcohol action plan. For example, it is unclear what the term “industry partners’ contribution…” means and who it means. WHO should not extend the remit of the dialogue to industry front groups.
The alcohol industry also has a fundamental conflict of interest with regards to data collection and WHO should primarily rely on official government data, not industry data.
Flaw #3: The Global Alcohol Action Plan fails to replace flawed concept of “harmful use of alcohol”
The Global Burden of Disease study 2018 showed that there is no safe level of alcohol consumption. The concept “harmful use of alcohol” is thus not compatible with evidence that has developed since the publication of the WHO GAS in 2010.
The concept of “harmful use of alcohol” however contributes to confusion about the origin of alcohol harm (it is the alcoholic products and industry practices, not the individual user) and about the perceived health benefits of alcohol use. Latest evidence shows that there is no positive effect of alcohol use, only negative and even small amounts of alcohol are harmful and increase the risk of developing cancer.
For public health promotion it is important to increase recognition of this risk through correct language, accurate information, labelling, campaigns, and other means.
Movendi International advocacy asks:
The draft global action applies the latest scientific evidence and the term “harmful use” be updated to “alcohol use” and/or “alcohol harms”.
Examples of problematic content:
- The word “harmful” is used 119 times throughout the document, making it one of the most used terms in the alcohol action plan.
- Notably, OP3 (page 2) defines “harmful use of alcohol” in line with the definition of the WHO Global Alcohol Strategy and refers to ICD-10 that also uses the same concept but with a different definition.
- OP4 highlights the confusion and lack of clarity in what “harmful use of alcohol” entails as concept.
- Action area 4, action 8 (WHO Secretariat): what is “harmful drinking” as opposed to “harmful use of alcohol”? This reflects inaccuracy of terms.
Positive elements of proposed action plan
Positive element #1: Increased ambition and commitment with focus on country impact
The last 10 years are a lost decade for alcohol policy action to protect more people and communities from the harms caused by the products and practices of the alcohol industry. That is why ambitious targets and bold actions are needed in the global alcohol action plan – especially through the alcohol policy best buys to facilitate impact on the country level.
Movendi International advocacy asks:
An ambitious target to reduce overall alcohol use in countries by 30% until 2030 is needed.
Improvement of targets in each action area to improve logic, coherence, and ambition.
An even more ambitious focus on and investment in advancing the three alcohol policy best buys to improve countries’ alcohol policy action is needed in the action plan.
An even more ambitious focus on and investment in advancing the three alcohol policy best buys to improve countries’ alcohol policy action is needed in the action plan.
Strong support for SAFER, WHO’s technical blueprint for alcohol policy development.
Increased commitment to technical capacity building for more countries to advance alcohol policy development.
Examples of positive content:
- Global targets 1.1 and 1.2, and 4.1
- Action area 1: Action 3 (Member States) and action 1, 3, 4, 6 (WHO Secretariat)
- Action area 4: Action 1, 2 (Member States) and action 3 and 5 (WHO Secretariat)
- Action area 6: Action 2 (Member States)
The language of the action is robust about the alcohol policy best buys, including alcohol taxation, and the commitment to technical support for member states.
Implementation of the three best buys would result in a return on investment of more than $8 for every $1 invested. Already in 2010, the World Health Report outlined that: “Raising taxes on alcohol to 40% of the retail price could have an even bigger impact [than a 50% increase in tobacco taxation]. Estimates for 12 low-income countries show that consumption levels would fall by more than 10%, while tax revenues would more than triple to a level amounting to 38% of total health spending in those countries.“ And the recent OECD report also contributed new evidence about the impact of the alcohol policy best buys. It outlines the triple dividend of preventing alcohol harm.
Positive element #2: Build a better, more sustainable, and functional alcohol policy infrastructure
According to the analysis of Movendi International, the current weak, flawed, and inadequate global infrastructure for alcohol policy development is one reason for the lack of progress in the last decade.
The platforms, networks, mechanisms of exchange and leadership for alcohol policy on global, regional, and national level need development and strengthening. This will facilitate alcohol policy mainstreaming and ensure greater attention across policy areas for alcohol policy solutions.
Movendi International advocacy asks:
Global day/ week to raise awareness about alcohol harm and policy solutions,
Global ministerial conference on alcohol under the guidance of WHO – like there is for mental health, for ending tuberculosis or for road safety for example,
Global inter-agency initiative to support Member States in the development of public health oriented alcohol taxation,
Functioning international network of alcohol focal points, and
Institutionalized permanent coordinating entity within national governments for alcohol policy consisting of senior representatives from all relevant departments of government as well as representatives from civil society
Examples of positive content:
- Action area 1: Action 5 (Member States) and Action 5 (WHO Secretariat)
- Action area 2: Action 5 and 10 (Member States) and Actions 1 and 9 (WHO Secretariat)
- Action area 3: Targets 3.1 and 3.2 as well Actions 2, 4 (Member States) and Actions 1, 3 (WHO Secretariat)
- Action area 4: Action 2 (WHO Secretariat)
These infrastructure elements are critically important for a more functional, sustainable, and fit-for-purpose alcohol policy infrastructure on all levels. This is needed for countries to learn from each other, support one another, exchange best practices, and collaborate across borders.
- Launching a global ministerial conference remains and important building block of fit-for-purpose infrastructure. Movendi International calls on Member States to take the lead.
- The action contains a strong mandate for the WHO Secretariat to advance an inter-agency initiative for supporting member states in the development of public health oriented alcohol taxation. Movendi International calls on WHO and other international organization to make use of that mandate.
Fit-for-purpose infrastructure will generate much needed momentum, facilitate synergies, and raise the level of alcohol policy commitment, leadership, and action.
Positive element #3: Convening an Expert Committee
Movendi International members welcome the proposal to reconvene the WHO Expert Committee on Problems Related to Alcohol Consumption.
Movendi International advocacy asks:
The remit of the Committee should be expanded to include providing recommendations on the way forward.
A specific timeline for the convening of the WHO Expert Committee on Problems Related to Alcohol Consumption should be specified.
Ensure participation in the expert committee from Knowledge Hubs, Collaborating Centers, and organizations in Official Relations with WHO.
Examples of positive content:
- Action area 4, action 11 (WHO Secretariat), including language on “providing recommendations on the way forward, and ensure the convening of regular meetings…”
When WHO “reconvenes” the expert committee, Movendi International calls for inclusion of broader set of participants to cover the entire field of expertise in the response to the global alcohol burden – as is already the case in other WHO expert committees.
Movendi International also requests a specific timeline for the convening of the WHO Expert Committee on Problems Related to Alcohol Consumption.
7 key messages and advocacy priorities
In surveys, studies, and anecdotes from around the world we see, hear, and experience that the health and well-being of children and youth is the most important value for people. But not just since the pandemic, the well-being of our children and youth is at risk and deteriorating. One big but often ignored reason is the products and practices of the alcohol industry.
- Alcohol is the 2nd largest risk factor for disease in the age group 10-24 years .
- Alcohol is the biggest risk factor for disease in the group 25-49 years.
- In 2016, the alcohol industry made more than $17 billion from under-age alcohol use.
In this context, Movendi International welcomes and endorses the WHO draft Global Alcohol Action Plan. The draft alcohol action plan contains several important elements to accelerate action on alcohol as public health priority, such as more ambitious targets, focus on the alcohol policy best buys and SAFER, and improvements of the infrastructure at all levels.
Movendi International welcomes and endorses the WHO draft Global Alcohol Action Plan. It contains several important elements to accelerate action on alcohol as public health priority, such as more ambitious targets, focus on the alcohol policy best buys and SAFER, and improvements of the infrastructure at all levels.”
Kristina Sperkova, International President, Movendi International
But our members remain concerned about serious flaws in the action plan. For example, the word “community” is mentioned only 9 times. The term “economic operators” however is mentioned three times more and addressed in every action area. Alcohol industry friendly concepts such as “harmful use of alcohol” and “self- and co-regulation” live on, despite the harm they contribute to and the confusion they cause. The WHO dialogue with the alcohol industry continues to undermine FENSA rules.
At the same time the global alcohol action plan contains several important elements to accelerate action on alcohol as public health priority – which Member States have called for in the decision at EB146.
- The target of a 20% reduction of per capita alcohol consumption is crucial to catalyze evidence-based public health action and reach the alcohol-related SDGs.
- A strong focus on the alcohol policy best buys and the SAFER initiative in the action plan will accelerate positive country impact to protect more people from alcohol harms. Best practice example in almost all WHO regions demonstrate the positive impact on health, economy, and development when countries implement the alcohol policy best buys.
- The way forward, paved by the global alcohol action plan, also needs investments in the global, regional, and national alcohol policy infrastructure. The draft contains important elements, but more should be done. We call for an inter-agency initiative to support countries in the development of alcohol excise taxation. And it is time for a global ministerial conference on alcohol policy to continue build momentum and leadership.
- The last 10 years since the adoption of the WHO Global Alcohol Strategy have been a lost decade for alcohol prevention and control. To ensure more attention and maintain much needed momentum, regular review at the WHO governing bodies about the progress of implementing the action plan is essential. A mechanism that facilitates biannual review of progress or lack thereof at the WHO governing bodies is important and should be included in the decision.
- We remain concerned about alcohol industry interference on all levels. In the consultation process, the alcohol industry mobilized tobacco industry affiliates, highlighting the need for WHO to better use FENSA protection concerning the alcohol industry. The draft action plan still affords a role to the alcohol industry, still maintains WHO’s dialogue with the alcohol industry, and still maintains the flawed and outdated concept of “harmful use of alcohol”. These are serious shortcomings of the alcohol action plan and might jeopardize urgently needed action to protect people from the harms caused by the alcohol industry.
- In this context of aggressive alcohol industry interference and persisting lack of protection measures, the task of the proposed expert committee to provide recommendations on the way forward is most welcome.
- Alcohol policy solutions hold substantial potential to improve health and help achieve the SDGs. To unlock the full alcohol policy potential, the rights and needs of people and communities affected by alcohol harm need to be placed at the center of action.
Movendi International statement(s)
Movendi International will make a statement on the global alcohol action plan. Please see the full statement here. We will deliver a shorter version of just one minute during the EB150 session.

FENSA applied? Alcohol and tobacco industry interference exposed
Brand new analysis shows that alcohol companies and their lobby groups are systematically working to undermine and water down global alcohol policies that would prevent and reduce the harms associated with their products.
The report from the Centre for Alcohol Policy Research (CAPR) at La Trobe University, released by the Foundation for Alcohol and Research Education (FARE), found that Big Alcohol deliberately worked to water down the World Health Organization’s (WHO) draft Global alcohol action plan 2022-2030 to strengthen implementation of the WHO Global Alcohol Strategy (the Action Plan).
The alcohol companies and their lobby groups made 60 submissions to the consultationon the Action Plan, making up nearly a quarter (24 per cent) of all submissions.
Many of these submissions made misleading claims and misrepresented evidence in an attempt to cast doubt on public health measures that are proven to prevent and reduce the harms from alcohol. The analysis found:
- Nearly all these submissions (90%) called for greater alcohol company involvement as a stakeholder/partner in reducing alcohol harms and policymaking;
- More than half (56%) of the submissions cast doubt on the WHO ‘SAFER’ initiative – evidence-based policies that target the price, availability and promotion of alcohol products, as well as policies to improve health services and prevention of driving under the influence of alcohol.
The report also found that only 36% (17) of these submissions referenced any specific evidence to support their arguments, and of these, ten misinterpreted the evidence, and nine promoted weak evidence.
FARE compared the Working Document and final draft of the Global Action Plan now before the EB150 and found changes consistent with recommendations made by alcohol companies and their lobbyists, including:
- A decreased emphasis on implementing the SAFER initiative – evidence-based policies that target the price, availability and promotion of alcohol products, as well as policies to improve health services and prevention of driving under the influence of alcohol, and
- Changing actions relating to alcohol marketing, enabling alcohol companies to set their own standards and rules rather than governments.
Research analysis found that WHO’s consultative processes for developing the Global Alcohol Action Plan have not been adequate to address conflicts of interest in relation to the alcohol industry, violating the principles of FENSA.
The alcohol and tobacco industries have used the extensive consultation period to undermine the process to develop the action plan and to water down the content of the plan.
As first exposed by Movendi International, organizations with known links to the tobacco industry participated in both web-based consultations, despite FENSA’s principle of non-engagement with tobacco industry actors.
Member States must ensure that WHO has the resources to implement and is held accountable for appropriate and consistent safeguards against industry interference in the development of global alcohol policy.
In a recent study, researchers analyzed the alignment of WHO’s consultative processes with non-state actors on the global alcohol action plan with FENSA. The researchers referred to publicly accessible WHO documents.
The researchers found that WHO’s processes to conduct due diligence, risk assessment and risk management as required by FENSA was inadequate.
Limited information was published on non-state actors, primarily the alcohol industry, that participated in the consultations, including their potential conflicts of interest. No minutes were published for WHO’s virtual meeting with the alcohol industry, suggesting a lack of transparency.
Organizations with known links to the tobacco industry participated in both web-based consultations, despite FENSA’s principle of non-engagement with tobacco industry actors.
Alcohol policy mainstreaming: other EB150 agenda items with alcohol policy implications
There are other EB150 agenda items linked to alcohol policy:
- The global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections,
- Global strategy for tuberculosis research and innovation,
- Strengthening WHO preparedness for and response to health emergencies,
- Strengthening WHO preparedness for and response to health emergencies,
- Interim report of the Working Group on Strengthening WHO Preparedness and Response to Health Emergencies,
- Public health emergencies: preparedness and response, WHO’s work in health emergencies,
- Maternal, infant and young child nutrition: Comprehensive implementation plan on maternal, infant and young child nutrition: biennial report,
- WHO global strategy for food safety,
- WHO reform: Involvement of non-State actors in WHO’s governing bodies.
ISSUE BRIEF EB150 WHO GLOBAL ALCOHOL ACTION PLAN
Download the PDF version of the Issue Brief about the global alcohol action plan at the 150th WHO Executive Board.